-oral anti-coagulant
-prolongs the PT --> extrinsic pathway
-monitor with INR
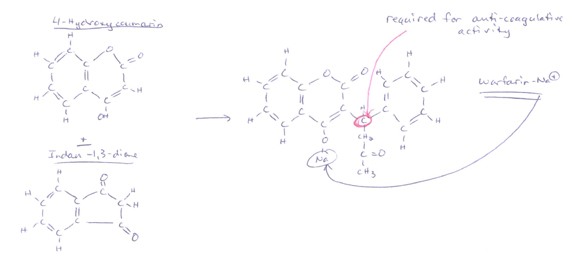
-Structure:
-synthesized from 4-Hydroxycoumarin & Indan-1,3-dione
-Mechanism:
1) Vit. K antagonism
2) Decreases levels of Proteins C & S (minor pro-coagulatory effect)
-Factors II (Prothrombin), VII, IX & X are made in the liver
-then acquire Gla residue (binds calcium (Factor IV)) --> neccessary for pro-coagulant activity
-the acquisition of the Gla residue step requires:
1) O2
2) CO2 &
3) Vit. K --> warfarin inhibits this
-Proteins C & S are also made in the liver but are only pro-coagulant if deficient --> normally anti-coagulative
-therapeutic doses:
1) decrease levels of each Vit. K-dependent coag factor by 30%-50%
2) decrease activity by 10%-40% of normal
-has no effect on fully carboxylated factors --> already completely synthesized
-so effex take time --> continue heparin for 4-5 days to allow coumadin levels to become therapeutic
-each affected coag factor has a different 1/2-life:
A) II (Prothrombin) --> ~50 hrs.
B) VII --> ~6 hrs.
C) IX --> ~24 hrs.
D) X --> ~36 hrs.
E) Protein C --> ~8 hrs.
E) Protein S --> ~30 hrs.
-may take several days to achieve full therapeutic anti-thrombotic levels --> continue heparin for 4-5 days
-even though the PT may be prolonged quickly (due to decreased levels of shorter 1/2-life coag factors Ex.) VII --> 6 hrs.)
-Dosing:
-Initial: --> 5 mg QD (PO or IV) x 2-4 days --> for pts. < 80 kg.
then 2 mg - 10 mg QD as indicated by INR monitoring
-may give 7.5 mg QD as initial dose for pts. > 80 kg.
-Absorption:
-bioavailability --> nearly complete w/ PO, IV, IM or rectal admin
-food in GI tract --> decreases PO uptake
-levels detectable w/in 1 hr.
-peak plasma concentration --> 2-8 hrs.
-Distribution:
-99% plasma protein bound (Ex.) albumin)
-0.14 L/kg
-fetal plasma levels approach maternal plasma levels --> contraindicated in pregnancy
-not found in breastmilk
-Elimination:
-inactivated in liver via cyto P450 CYP2C9 --> caution in hepatic dis.
-excreted in urine & stool (renal & GI clearance)
-clearance rate = 0.045 mL/min x kg
-1/2-Life:
-25-60 hrs.
-Duration Of Action (DOA):
-2-5 days
-Drug Interactions:
-MANY --> esp. w/ cyto P450 altering drugs
-Other Interactions:
1) Green leafy vegetables
-high in Vit. K --> antagonizes coumadin's effex --> will shorten the PT
2) Some Abx
-decrease GI synthesis of Vit. K --> will further prolong the PT (additive effex)
3) Impaired Hepatic Function
-will decrease Vit. K-dependent factors --> additive effex to further prolong the PT
4) CHF
-will decrease Vit. K-dependent factors --> additive effex to further prolong the PT
5) Hyperthyroidism
-will decrease Vit. K-dependent factors --> additive effex to further prolong the PT
6) Age
-increased sensitivity to warfarin dosing with increased age
-Resistance:
-some pts. require > 20 mg QD to achieve therapeutic INR's (2.0 - 3.0)
-usually due to excessive dietary Vit. K intake (diet &/or supplements) --> not true resistance
-10% of pts. require < 1.5 mg QD to achieve therapeutic INR's (2.0 - 3.0)
-pts. just very sensitive --> not resistant
-due to variant cyto P450 CYP2C9 enzmye --> inefficient inactivation of warfarin
-affex 10%-20% of caucasian Amers.
-affex < 5% of african Amers. & native Amers.
-Hereditary Warfarin Resistance:
-a rare d/o in which pts. have a mild depression of Vit. K-dependent coag factor biosynthesis
-Side Effex:
1) Bleeding:
-increased risk w/ increased dose & duration of tx.
-~5% / yr risk w/ pts. w/ INR's of 2.0 - 3.0 (therapeutic levels)
-increased risk of intracranial hemorrhage w/ INR > 4.0
2) Elevated INR:
2.0-3.0:
-~5%/yr risk of serious bleed
>4.0:
-increased risk of intracranial bleed
< 5.0 but > therapeutic range:
-d/c Warfarin (Coumadin) until INR drops down to therapeutic range
transiently > 5.0
-usually due to a new med (Ex.) Acetaminophen) or change in meds regimen (esp. cyto P450 CYP2C9 inhibitors --> decreased Warfarin (Coumadin) breakdown
5.0 - 9.0
-Give 1.0 mg - 2.5 mg Vit. K PO*
9.0 - 20.0
-Give 3.0 mg - 5.0 mg Vit. K PO*
> 20.0
-Give FFP (10-20 mL/kg) immediately plus 10 mg Vit. K slow IV*
* -Vit. K admin will make pts. unresponsive to Warfarin (Coumadin) for several days
-Vit. K admin will take 24-48 hrs. to decrease INR's to therapeutic ranges b/c takes time to synthesize new coag factors
-May use Heparin instead for continued anit-coagulation
3) Skin Necrosis:
-appears 3-10 days after initial tx
-most commonly:
A) on extremities
B) in Protein C deficiency --> hypercoagulable state
-Protein C has short 1/2-life --> ~8 hrs.
-functional activity falls more rapidly w/ initial Vit. K antagonist dose
4) Purple Toe Syndrome:
-may develop 3-8 wks. after initial tx.
-caused by cholesterol emboli release from plaques
5) Alopecia
6) Urticaria
7) Dermatitis
8) Fever
9) N / V / D
10) Anorexia
11) Abd. cramps
12) HIT:
-venous limb gangrene
-if pt. is HIT-Ab positive --> use Lepirudin (Refludan) or Danaparoid (Orgaran)
-Contraindications:
-Pregnancy:
-crosses the placenta --> fetal plasma levels approach maternal levels
-causes birth defex & abortion (even w/ PT levels in the low therapeutic range)
-if ingested in:
A) 1st trimester --> nasal hypoplasia or stippled epiphyseal calcifications
B) 2nd or 3rd trimester --> CNS abnormalities
-use heparin instead --> does NOT cross the placenta
-Lab Monitoring:
-INR (International Normalized Ratio) --> measures PT efficacy
-most indications for chronic oral anti-coagulation --> INR of 2.0 - 3.0
-higher for pts. w/ mechanical heart valves
INR = (patient PT / reference PT) ISI
-where ISI = International Sensitivity Index --> supplied by manufacturers
-coumadin requires QD lab monitoring w/ INR's until INR is therapeutic --> then weekly INR's --> then monthly INR's
-INR NOT useful in SLE --> lupus anti-coagulant
-pt. already has prolonged PT @ baseline
-use anti-factor Xa assay to monitor instead
-Uses:
1) Prophylaxis & prevention of progression of:
A) Acute DVT
B) PE
-following an initial course of heparin
-continue heparin x 4-5 days to allow therapeutic levels to come about
-therapeutic levels --> INR in therapeutic range on 2 consecutive days --> then weekly INR's --> then monthly INR's
2) Prevent venous thromboembolism in:
A) Acute MI
B) Prosthetic heart valves
C) Chronic AFib
=================================
References:
Goodman & Gilman's: The Pharmacologic Basis Of Therapeutics - 10th Edition - 2001. Chapter 55.